Agnė Pašvenskaitė1, Deimantė Bajoriūnaitė2, Roberta Buginytė2, Virgilijus Ulozas1
1 Lithuanian University of Health Sciences, Department of Otorhinolaryngology, Kaunas, Lithuania
2Lithuanian University of Health Sciences, Academy of Medicine, Kaunas, Lithuania
Abstract
Background. Laryngeal tuberculosis is a rare form of tuberculosis that usually develops due to direct spread from a bronchus or hematogenous spread. The most common symptom related to laryngeal tuberculosis is hoarseness which also can be led by dysphagia, odynophagia, cough, or nonspecific symptoms like fever or localized pain. To confirm laryngeal tuberculosis, histopathologic examination is necessary because it can mimic laryngeal cancer. Diagnosis of laryngeal tuberculosis is made through a combination of a comprehensive otorhinolaryngological examination, imaging, laboratory and histological analysis.
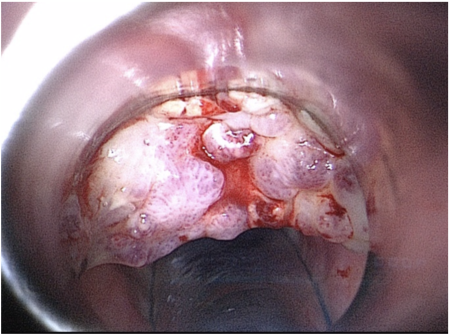
Case report. We describe the case of a 62-year-old Lithuanian man who presented with the clinical picture of laryngeal cancer, but which turned out to be tuberculosis. We illustrate the difficulty of recognizing laryngeal tuberculosis both clinically and even with radiological examination.
Discussion. Laryngeal tuberculosis is a rare condition that can mimic laryngeal cancer. In male patients with a history of smoking and complaining of dysphonia, odynophagia, and cough LT is a diagnosis to be considered.
Keywords: Laryngeal tuberculosis, tuberculosis, dysphagia, odynophagia, cough.