Eglė Bakučionytė 1, Iveta Idzelytė 2, Miglė Ivanauskaitė 2
1 Republic Hospital of Klaipeda, Klaipeda, Lithuania
2 Lithuanian University of Health Sciences, Academy of Medicine, Faculty of Medicine, Kaunas, Lithuania
ABSTRACT
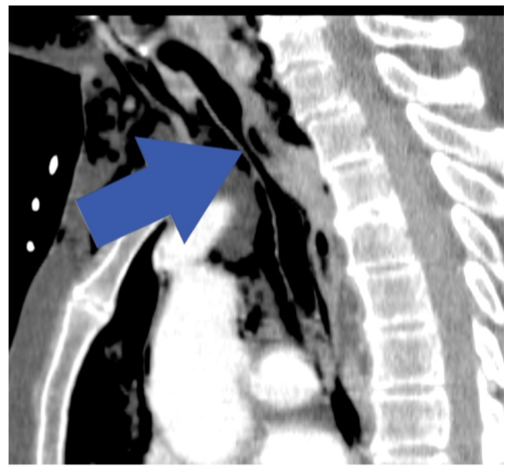
Tracheal rupture is a rare iatrogenic complication of endotracheal intubation that occurs only in 1/20,000-75,000 patients. This condition requires prompt diagnosis and treatment because of high morbidity and mortality. We present a case report of a 81-year-old woman that presented with subcutaneous emphysema just after modified radical mastectomy.
Keywords: tracheal rupture, endotracheal intubation, pneumothorax, pneumomediastinum, subcutaneous emphysema.