Iveta Idzelytė 1, Tomas Lobinas 2, Vestina Strakšytė 2
1 Lithuanian University of Health Sciences, Academy of Medicine, Faculty of Medicine
2Department of Radiology, Hospital of Lithuanian University of Health Sciences Kaunas Clinics
Abstract
Background: sigmoid volvulus is a cause of large bowel obstruction and occurs when the sigmoid colon twists on its mesentery. This condition requires prompt diagnosis and treatment for better disease outcomes. According to the literature, sigmoid volvulus typically develops in patients of an older age with other comorbidities.
Aim: to present a clinical case of SV and review the latest scientific literature, and to raise awareness of this life-threatening disease, which can be successfully treated due to timely diagnosis.
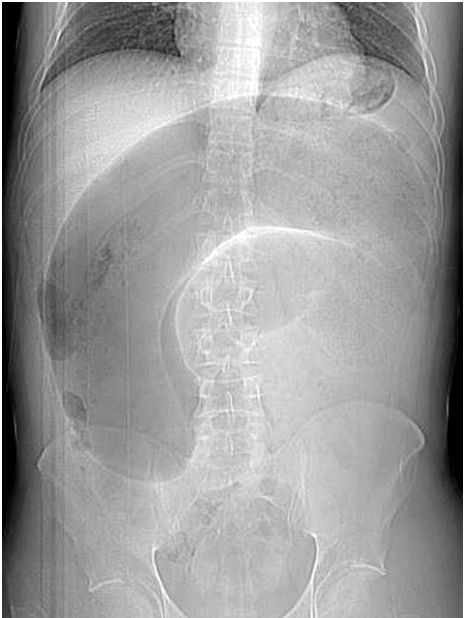
Methods: We presented a case report of a 33-year-old man with a sigmoid volvulus. After surgical treatment, the histopathological examination revealed Hirschsprung’s disease. Publications, researching the problem of sigmoid volvulus, were reviewed.
Conclusions: sigmoid volvulus is a life-threatening disease and radiological signs have an important value diagnosing this pathology and may help to determine the therapeutic approach. Plain abdominal radiography and CT are widely available diagnostics tools for making correct SV diagnosis.
Keywords: sigmoid volvulus, Hirschsprung’s disease, radiologic features.