Viktor Migunov1
1Vilnius University, Faculty of Medicine
Abstract
Background. Invasive pulmonary aspergillosis is a life-threatening fungal disease and usually affects immunocompromised patients. Clinical symptoms and radiological findings are nonspecific and may be indistinguishable from other pulmonary conditions such as pneumonia or pulmonary tuberculosis. Invasive pulmonary aspergillosis is a rare condition in patients with solid tumours and is usually not considered.
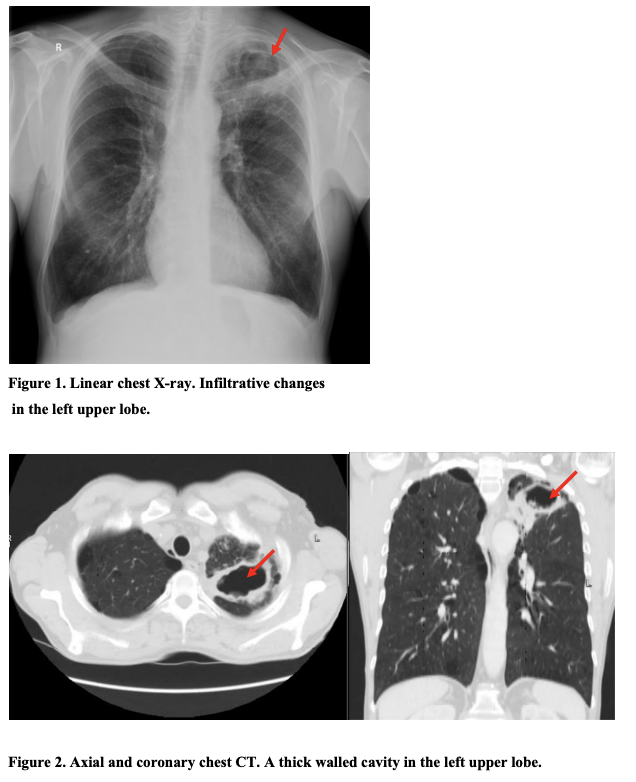
Case report. In this case a 58-year-old man was misdiagnosed with pneumonia. After he failed to respond to antibiotic treatment, pulmonary tuberculosis was suspected. Final diagnosis was invasive pulmonary aspergillosis and lung adenocarcinoma. This case illustrates the challenges of recognizing invasive pulmonary aspergillosis.
Discussion. Diagnosis of invasive pulmonary aspergillosis is challenging and requires a combination of clinical, radiological and microbiological features. Diagnostic methods and accuracy in recognizing invasive pulmonary aspergillosis can differ and depend on patients clinical features.
Keywords. Aspergillus, invasive pulmonary aspergillosis, tuberculosis, lung adenocarcinoma.